Muscle biopsy is mainly used in the investigation of neuromuscular disease. Pertinent clinical signs that might trigger the need for a muscle biopsy are outlined in Fig 2 (not an exclusive list). A muscle biopsy allows evaluation of myofibres, intramuscular nerve branches, surrounding connective tissue and blood vessels. It can be particularly helpful in distinguishing primary muscle disease from primary neurological disease.
Fig 1. Muscle structure: Muscles comprise multiple fascicles composed of multiple myofibres (pink) separated by endomysium (pale green) and ensheathed by perimysium (purple). Myofibres are individual muscle cells and they contain actin and myosin, responsible for contraction.
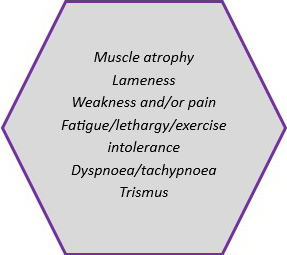
Fig 2. Common reasons to pursue muscle biopsy
a) Sample the same three muscles routinely, provided they are affected by the disease process. Suggested muscle are the triceps, cranial tibialis and a muscle of mastication, particularly temporalis or masseter†. They are easy to access surgically and allow evaluation of several sites. Since they are more commonly assessed, their normal morphology is better characterised which makes interpretation more reliable.
b) Avoid terminally affected muscle that may be completely atrophied or replaced by scar tissue. Also avoid sampling too close to a site of tendon insertion.
c) Sample size: Aim for approximately 1cm3 from each site sampled; this requires open muscle biopsy rather than a percutaneous needle biopsy. Needle biopsies are really too small for use in general veterinary diagnostic pathology.

a) Place in 10% neutral buffered formalin. Some authors recommend pinning muscle to cardboard to keep the muscle straight and avoid fixation artefact (muscle can contract when placed in formalin). This is not critical, however.
b) Place different sample sites in different pots and label the pots.
c) Consider submitting samples to a specialist neuromuscular pathology laboratory (Fig 3). If you do this, try to contact the laboratory ahead of time for submission advice.
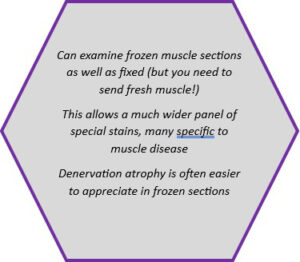
Fig 3. Advantages of specialist neuromuscular laboratory
*Other clinical information helpful in muscle disease investigation:
- Areas of the body affected; localised or generalised
- Age of onset
- Duration of clinical signs
- Progressive or not; waxing and waning?
- Response to any treatment
† Inflammation in a muscle of mastication could be due to masticatory muscle myositis but it could also be a localised manifestation of polymyositis. Sending muscle biopsies from different sites can help to separate these, preferably alongside type IIM serology.
Related Posts

Oncology Service Now Available – FREE for 3 months
Download a PDF

2026 Bank Holiday Information
Download a PDF
Organ of the Month: Muscle
Organ of the month: Muscle I. Muscle biopsy In this blog, we turn to muscle…
Organ of the Month: Mammary Glands
Organ of the month: Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among…