Related Posts

July 1, 2026
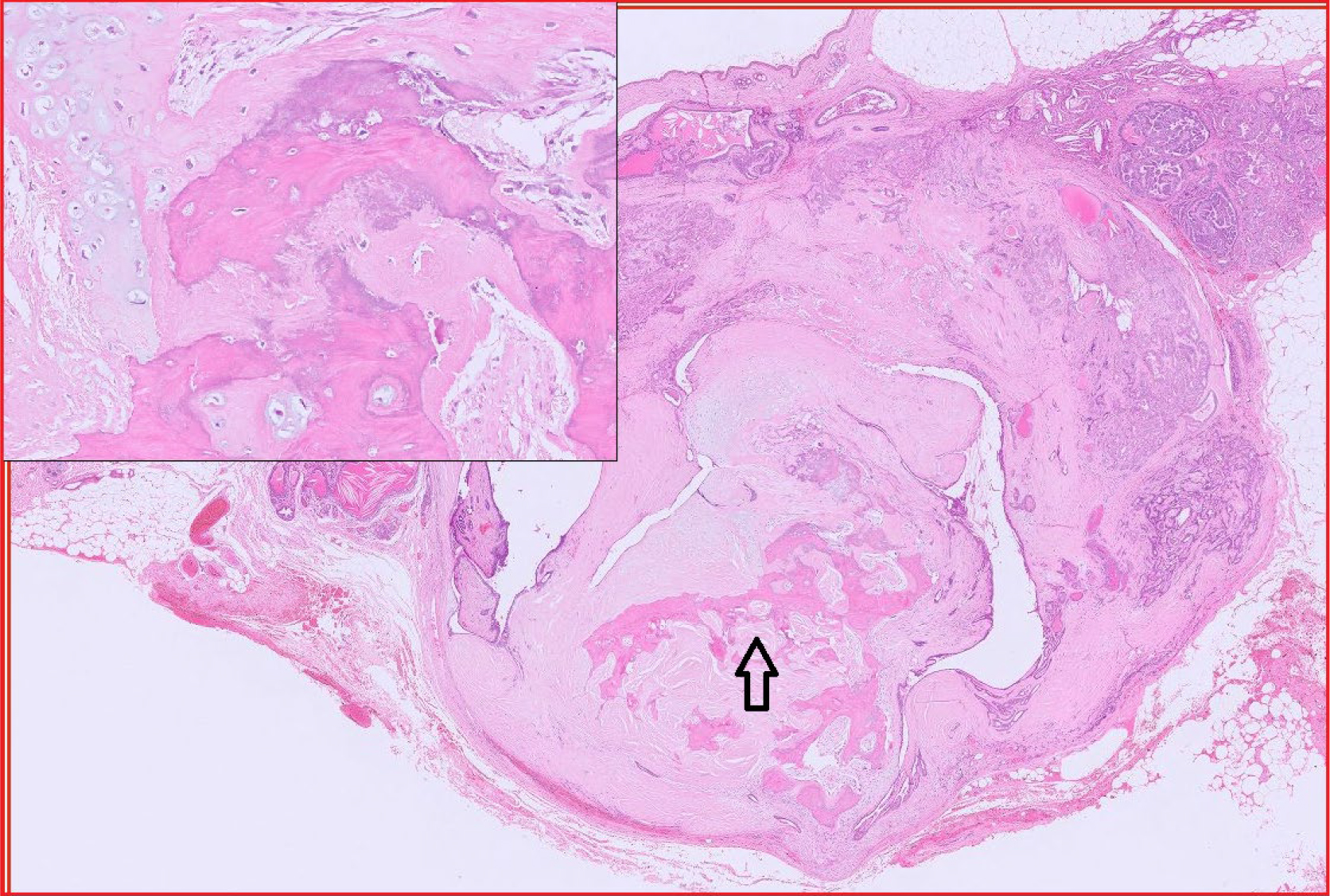
Organ of the Month: Bone
Organ of the month: Bone I. Indications for bone biopsy. A. Bone tumours Do –…
April 16, 2026
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in Veterinary Cytology
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…

February 27, 2026
2026 Bank Holiday Information
Download a PDF

February 25, 2026
Organ of the Month: Muscle
Organ of the month: Muscle I. Muscle biopsy In this blog, we turn to muscle…