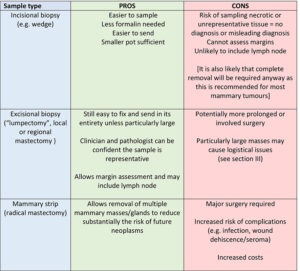
Table 1. Pros and cons of various mammary gland sampling methods
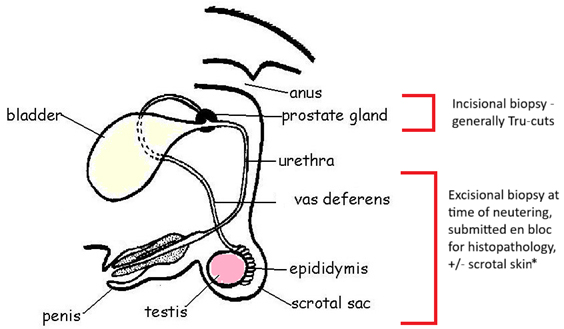
To assist with orientation (see Fig 1):
- Leave skin attached – this also helps with margin assessment.
- Large samples can be split into three or four pieces, e.g. a mammary strip could be divided into cranial, middle and caudal. Please make sure pots are clearly labelled. Photographs can be very helpful. We cannot discern cranial, caudal, left and right without clear indicators so, if this is important to you, please let us know. Bear in mind that, while a single large mass could be divided into, say, four quarters, this can make it difficult to identify margins post fixation.
- Send lymph node where possible (especially for cats) and let us know you have done this.
- pecific areas of interest can be marked with a suture.
- Also please refer to Finn Factsheet No. 91
Fig 1. Orientation tips for mammary strip
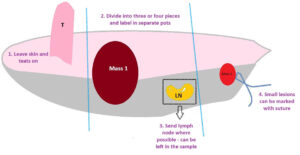
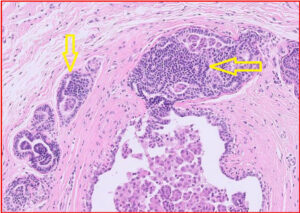
Fig 2. Complex mammary adenoma, canine – this contains both epithelial cells (top left inset) and myoepithelial cells (bottom right inset). This is one of the most common benign mammary tumours we see in the dog. It is well-demarcated and compressive – classical features of a benign neoplasm.
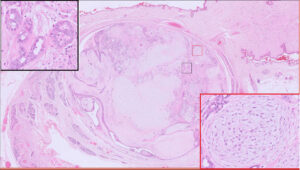
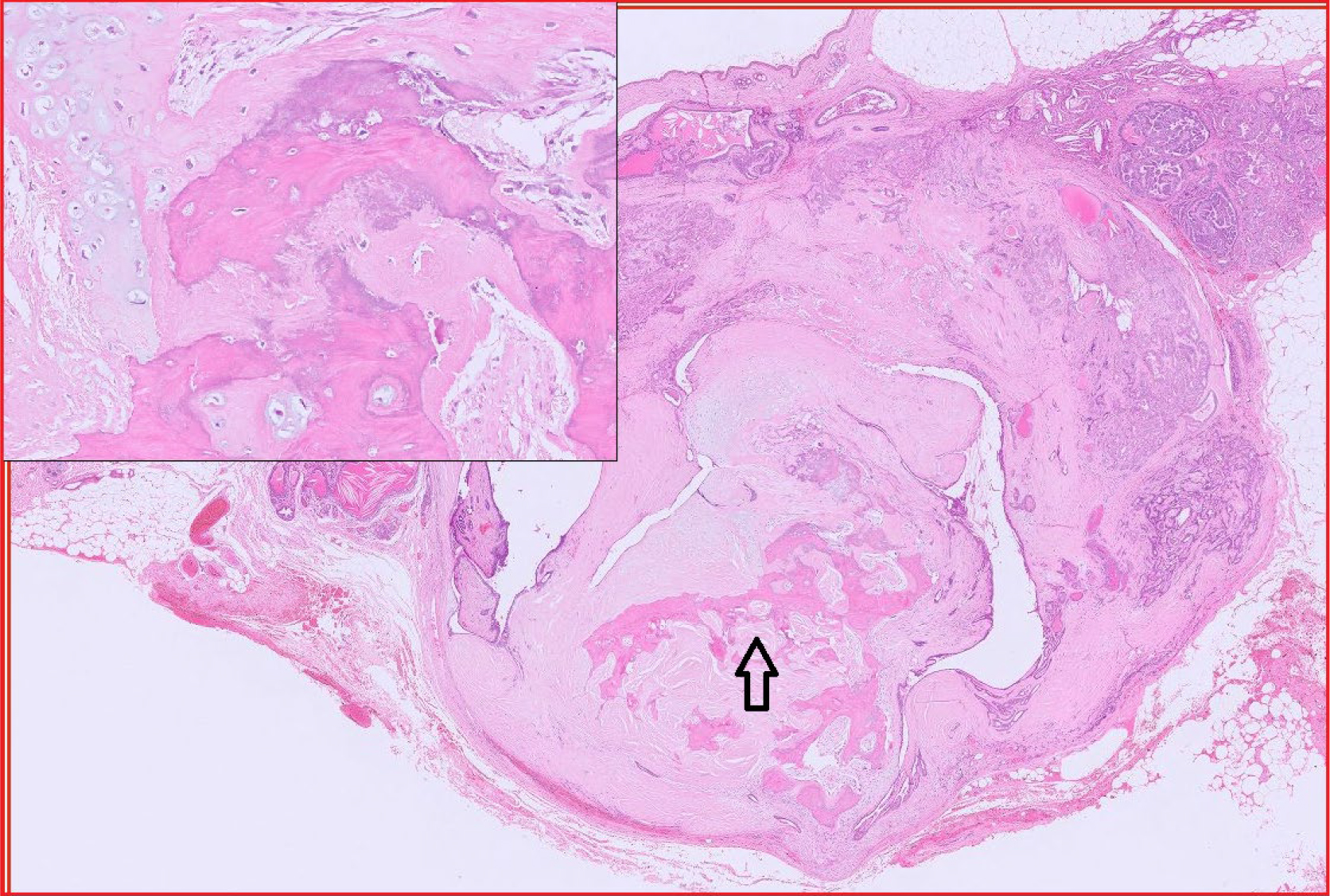
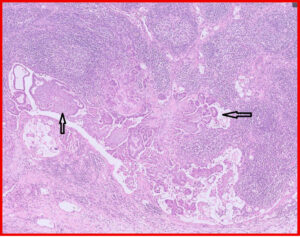
Fig 3. Benign mixed mammary tumour, canine. This is another common mammary tumour in the dog. It differs from the complex mammary adenoma in that it contains bone and/or cartilage (inset). Arrow = bone.
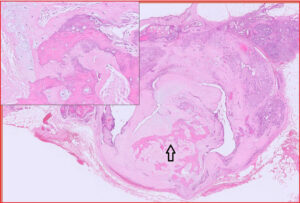
Fig 4. Mammary carcinosarcoma, canine. This is an uncommon mammary neoplasm that is unfortunately very aggressive. It is composed of epithelial and mesenchymal cells and both populations are malignant. The mesenchymal component can also produce osteoid and/or chondroid matrix, i.e. forming a chondrosarcoma or osteosarcoma. The epithelial cells metastasise via lymphatics vessels to regional lymph nodes and the lungs, while the mesenchymal cells spread haematogenously to the lungs. Much of this particular example is necrotic.
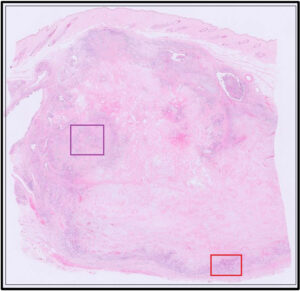
Fig 5. Red box from Fig 4, illustrating epithelial cells with features of malignancy (red arrowhead = mitoses; yellow arrowhead = multiple nucleoli). There is also a fairly high nuclear to cytoplasmic ratio, moderate anisokaryosis and nuclear atypia.
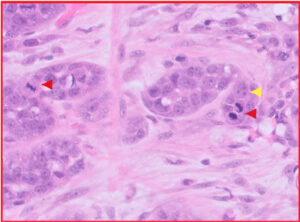
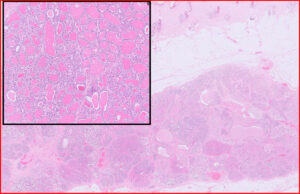
Fig 6. Purple box from Fig 4, illustrating mesenchymal cells and production of tumour-associated osteoid matrix (yellow arrows), sufficient for a diagnosis of “osteosarcomatous” differentiation within this carcinosarcoma.
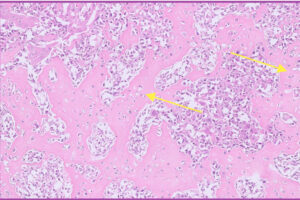
Fig 7. Higher magnification of neoplastic mesenchymal cells from Fig 6 above.
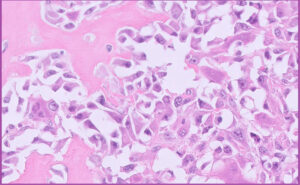
Fig 8. Feline mammary carcinoma (solid type with lots of necrosis).
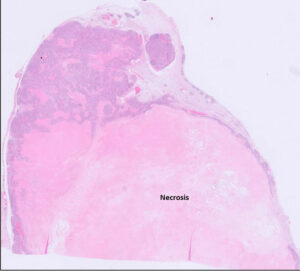
Fig 9. Same tumour as Fig 8 including lymph node. [Inset = lymphatic invasion]
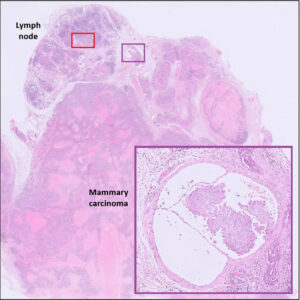
Fig 10. Red box from Fig 9. Neoplastic cells are present in the lymph node sinus, indicating metastasis (black arrows)
Figs 11A and B. Not all lesions are neoplastic.
11A: Mammary lobular hyperplasia, canine
11B: Mammary epitheliosis (yellow arrows), canine. This is believed to be a precursor to carcinoma.
In cats, one of the more common non-neoplastic lesions we see in the mammary area is duct ectasia, with or without inflammation. This can create a “spongy” texture within the mammary area. While we do see mastitis from time to time, this is much less common in companion animal species.
Related Posts

Oncology Service Now Available – FREE for 3 months
Download a PDF

2026 Bank Holiday Information
Download a PDF

Organ of the Month: Muscle
Organ of the month: Muscle I. Muscle biopsy In this blog, we turn to muscle…
Organ of the Month: Mammary Glands
Organ of the month: Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among…